Prof. dr hab. n. med. Paweł Lampe
Katedra i Klinika Chirurgii Przewodu Pokarmowego
Śląskiego Uniwersytetu Medycznego w Katowicach
Does it matter what a hospital is “high volume” for?
Specificity of hospital volume‐outcome associations for
surgical procedures: analysis of administrative data
Canada
„Under this interpretation, regionalisation of patients needing complex surgical
procedures to hospitals that do a high volume of those procedures would be
expected to improve patient outcomes regardless of the underlying causal
mechanism of the volume‐outcome association.”
„We found that the short term outcomes of some complex surgical procedures were
better in hospitals with a higher volume of the same procedure. However, we found
that in many cases outcomes were also better in hospitals with high volumes of
different procedures”.
Regionalizacja pacjentów wymagających kompleksowych zabiegów
chirurgicznych w szpitalach wykonujących dużą liczbę określonych
procedur daje lepsze wyniki i mniejszą liczbę powikłań.
Podobne wyniki osiąga się w szpitalach wykonujących dużą liczbę
różnorodnych procedur.
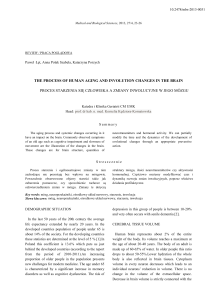
Hospital volume and mortality after pancreatic resection: a
systematic review and an evaluation of intervention in the
Netherlands.
FIGURE 2. Hospital mortality in the 4 volume categories at the different time
intervals (1994–1995, 1996–1998, 1999–2000, 2001–2003).PD‐pancreaticoduodenectomy
„….hospital mortality rates were between
13.8% and 16.5% in hospitals with less than 5 PRs per year, whereas hospital mortality
rates were between 0% and 3.5% in hospitals with more than 24 PRs per year.”
W szpitalach wykonujących mniej niż 5 pankreatoduodenektomii
rocznie śmiertelność szpitalna wynosi 13.8 – 16.5%
W szpitalach wykonujących ponad 24 pankreatoduodenektomie
rocznie śmiertelność szpitalna wynosi 0‐3.5%
Pancreatic cancer: Services to improve survival
UK
„To dobra decyzja dla pacjentów toczących walkę z tą śmiertelną
chorobą . Rak trzustki jest relatywnie rzadką chorobą, ale jedną z
najgorzej rokujących. Skuteczne leczenie wymaga
wysokospecjalistycznego klinicznego doświadczenia i sprzętu.
Aby to osiągnąć musimy tworzyć wiodące w regionie wyposażone
centra ekspertów
Desygnować centrum chirurgiczne
Inwestować w specjalistów,
kształcenie i badania
Opracowane wytyczne rekomendują jedno centrum chirurgiczne
leczenia raka trzustki przypadające na 2‐4 ml populacji
Centralisation of upper gastrointestinal cancer surgery
UK
Upper gastrointestinal surgery comprised of the separate disciplines of
oesophagogastric (OG) and hepato‐pancreato‐biliary (HPB) surgery includes the
Niezależnie
wyniku,
jest jasne,surgery.
że centralizacja
operative
care ofod
theostatecznego
most complex cancers
in alimentary
chirurgii górnego
odcinka
przewodu
pokarmowego
musieach
zaistnieć
Historically,
any given general
surgeon
would see
relatively few cases
year,
zgodnie
z silnymi
trendami.
resect even fewer
and outcomes
wereświatowymi
notoriously poor
Chirurgia górnego odcinka przewodu pokarmowego składa się z
Whatever
eventual outcome,
it is clear
that the
forces for
centralisation
upper
dwóchthe
odrębnych
dyscyplin:
chirurgii
przełyku
i żołądka
orazofchirurgii
gastrointestinal cancerwątroby,
surgery aretrzustki
potent and
global
in their scope.
i dróg
żółciowych.
W przeszłości chirurg ogólny mógł spotkać się z kilkoma przypadkami
tej chirurgii rocznie, jeszcze mniej przypadków mógł zoperować,
a rokowanie było bardzo złe.
The shape of provision continues to evolve but it is likely that the centralisation of
upper gastrointestinal cancer will produce profound alterations to the shape of ‘general
surgery’ across many healthcare systems
Przepisy się zmieniają, ale jest prawdopodobne, że centralizacja leczenia
raka górnego odcinka przewodu pokarmowego przyniesie głębokie
zmiany w kształcie "chirurgii ogólnej" w wielu systemach opieki
zdrowotnej
Surgeon Volume and Operative Mortality in the
United States
”Operative deaths were increased by
•24% following surgery for lung cancer,
•83% for surgery of bladder cancer,
•130% for surgery of esophageal cancer and
•361% for surgery of pancreatic cancer in patients who had a
surgeon who had performed a low‐volume of the specific procedure,
compared to those who had surgeon who had performed a high volume
of the procedure”.
W chirurgii trzustki, okołooperacyjne ryzyko zgonu rośnie do ok. 361%
jeżeli pacjent był operowany przez chirurga z mały doświadczeniem, w
porównaniu z chirurgiem, który wykonał
wiele zabiegów z tej dziedziny
Evaluating compulsory minimum volume standards in
Germany: how many hospitals were compliant in 2004?
Survival Following Curative Resection for Pancreatic Ductal
Adenocarcinoma.
A Systematic Review of the Literature
Irlandia
5 szpitali zaprzestało operowania raka trzustki, zabiegi przejął St.
Vincent´s Hospital w Dublinie.
Szpitale te wykonywały mniej niż 20 operacji raka trzustki rocznie.
Dear Professor Lampe, Thank you for your mail.
Indeed in each area in France there are Reference Centers where acute
pancreatitis,tumors of the pancreas and complications after
pancreatic surgery and abdominal surgery are treated. There is no real specific financial
support for these centers. Each hospital has a budget
and resources according to its activity. We call it "T2A" which means "budget according
to activity". This is in contradiction with the previous policy of "budget global"which
was a fixed budget independent of the real activity. Therefore a hospital with higher
volume of activity will automatically receive more financial support.
If you need more details do not hesitate to ask me. Merry Christmas also to you and
very Happy New Year !
With kindest regards
Daniel Jaeck
Hôpitaux Universitaires de Strasbourg Centre de chirurgie viscérale et de
transplantation
Hôpital de Hautepierre
Dear Professor Lampe,
Thank you very much for your mail. Regarding to pancreatic surgery ‐ this is only part of
general surgery in big hospital, nothing more. There is unfortunately only one way for
payment there ‐ this is health care insuraence company.
We have no chance to obtain more money for our care for patients with pancreatic
diseases.
Merry Christmas to you and to your family. Best wishes
Miroslav Ryska
prof. MUDr. Miroslav Ryska Chirurgická klinika
Ústřední vojenská nemocnice U Vojenské nemocnice 1200, Praha
The association between higher volume and better
outcome for pancreatoduodenectomy
Sweden
„It is becoming more and more difficult for general surgeons to defend their preserves
and to persist in undertaking pancreatoduodenectomy once in a while.
It is high time for us to pay regard to the higher volume–better outcome association
for this particular operation.”
Ingemar Ihse Department of Surgery University Hospital S‐221 85 Lund, Sweden
Coraz trudniejsze staje się dla chirurga ogólnego bronienie swoich racji
i celowości wykonywania sporadycznie pankreatoduodenektomii.
Nadszedł najwyższy czas na to, aby zdać sobie sprawę z lepszych
wyników tej operacji w ośrodkach wykonujących ich dużo.
Hospital Cost‐categories of Pancreaticoduodenectomy
Belgia
A Hundred Consecutive Pancreaticoduodenectomies in
India
Pancreaticoduodenectomy in specialized institutions in the USA and other western
countries carries a mortality of 3‐8%, a morbidity of 40%, a mean hospital stay of 14
days and an average expenditure of 20,000 dollars.
The average cost of operation was INR 118,000/‐(range 70,000/‐ to 374,000)
equivalent to US $ 2300.
Koszt pankreatoduodenektomii w USA i krajach Zachodniej Europy
wynosi 20000 dolarów.
W Indiach 2300 dolarów.
Materiał Kliniki
Pankreatoduodenektomie (Whipple, Traverso,
Claget, Flautner,Imanaga)
1990 ‐ 2007 rok
784 pacjentów
70
Liczba PD
60
50
40
30
20
36
27
10131 19 20
49 43
51
37
45 47 43
61 56
70 67
48 52
0
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008
Lata